
The Administration of Vitamin D from Childhood to Adult


Abstract
Introduction
The effects and implications of vitamin D in the development and proper functioning of the human body have been well studied, recognizing the importance of this vitamin in the absorption and normal use of calcium and phosphorus and maintaining normal calcium levels in the blood, maintaining bone and muscle health, and tooth structure, normal functioning of the immune system, cell division, obesity. Vitamin D doses are varying depending on body age and needs in the different accelerated growth periods of infancy, puberty and adolescence.
Methods
Given the major implications of vitamin D deficiency in pathology, the authors present 3 clinical cases that exemplify some of the roles of vitamin D.
Results
The first case is a 10-month-old infant, diagnosed with malabsorption syndrome, who also has associated vitamin-protein pluri-carential syndrome. The second case is an adolescent with joint and bone pain, which has been diagnosed with hipovitaminosis D and hypocalcaemia. The third case is a 9-year-old girl, known with obesity and respiratory allergy, in which routine biological evaluation found a major vitamin D deficiency.
Conclusions
Knowing the implications of vitamin D in the body and the sensitive periods of growth and development, it is important to make biological determinations of vitamin D levels, in order to do proper prophylaxis and intervene promptly when changes occur. Prophylactic doses of vitamin D will be adjusted depending on the patient’s individual characteristics and on the risk factors for the occurrence of different pathologies.
Table of contents
1. Introduction
2. Methods
3. Results
4. Conclusions
1. Introduction
The effects and implications of vitamin D in the development and proper functioning of the human body have been well studied, recognizing the importance of this vitamin in the absorption and normal use of calcium and phosphorus and maintaining normal calcium levels in the blood, maintaining bone and muscle health, and tooth structure, normal functioning of the immune system, cell division, obesity. Vitamin D doses are varying depending on body age and needs in the different accelerated growth periods of infancy, puberty and adolescence.
2. Methods
Given the major implications of vitamin D deficiency in pathology, the authors present 3 clinical cases that exemplify some of the roles of vitamin D.
The first case is a 10-month-old infant, who presented for low appetite, undernutrition, facial and thoracic lesions of atopic dermatitis and diarrhea, occurred for ~ 3 months, when breast- feeding stopped and received the milk formula.
Due to the fact that the infant is living in the temperate zone, he receives prophylaxis of rickets with usual doses of vitamin D. The complementary food was ovo-lacto- vegetarian, due to the parents’ beliefs.
The anthropometric assessment according to WHO Growth Chart (World Health Organization) has objected the underwheight (Z-score interpretation < -2). Following the investigations, the infant was diagnosed with Cow’s milk protein allergy, associating vitamin-protein pluri-carential syndrome.
The Biochemical Assessment of plasma 25-hydroxyvitamin D (25(OH)D) concentrations was performed in three stages; at the onset, after 2 months and 4 months of vitamin D therapy (Table
1), associated with appropriate diet-avoid milk and other dairy products, extensively hydrolysed milk formula (eHF), without lacotose initialy, then with lactose and correcting malnutrition.

The second case is a 15-year-old adolescent with joint and bone pain, palpitation, precordial pain, which has been diagnosed with hipovitaminosis D and hypocalcaemia Family and personal history does not reveal significant illness.
The adolescent practicing swimming twice a week, does not smoke, consume cigarettes, alcohol or drugs.
The nutrition is age-appropriate, with high consumption of vegetables and low milk and dairy products consumption; the sun exposure is minimum.
Over the past half year, it has experienced accelerated stature growth, which coincided with the onset of symptomatology.
The clinical examination reveals a good general status, weight and height corresponding to age according to the WHO growth charts, normal body mass index (BMI), without cardio-pulmonary manifestation, symmetric low back pain, muscle aches, and throbbing bone pain elicited with pressure over the tibia and positive Chwosteck sign.
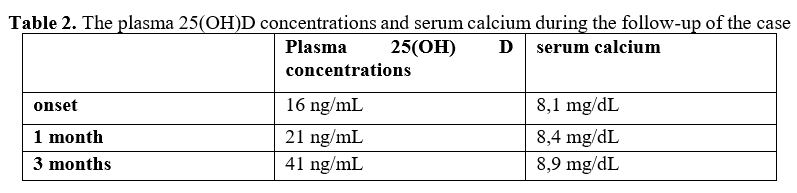
The biochemical assessment reveals low plasma 25-hydroxyvitamin D concentrations and hypocalcaemia, without hypomagnesemia and normal plasma parathyroid hormone concentrations [1].
The patient was clinically and biologically assessed at 1 month and 3 months after the onset (Table 2).
Bone densitometry (dual-energy x-ray absorptiometry or DEXA) does not show pathological changes (Z-scores at various skeletal sites). The cardiology examination did not detect’s pathological changes.
Other pathological entities that can generate the described symptoms have been clinically and biologically excluded.
The third case is a 9-year-old girl, known with obesity and respiratory allergy (allergic rhinitis and asthma), in which routine biological evaluation found a major vitamin D deficiency.
Family history reveals familial hypercholesterolemia and obesity on the maternal line, with high cardiovascular risk, and allergy on the paternal line. The patient did not benefit from breastfeeding; complementary nutrition was correctly introduced. The BMI-for-age WHO Growth Chart reveal a Z-score >1 until 3 years, a Z-score >2 at 5 years, then a Z-score >3. Weight gain has been linked to unhealthy lifestyle, the child being a major consumer of fastfood, sweets, in combination with reduced physical activity. The patient was evaluated to show obesity comorbidities.
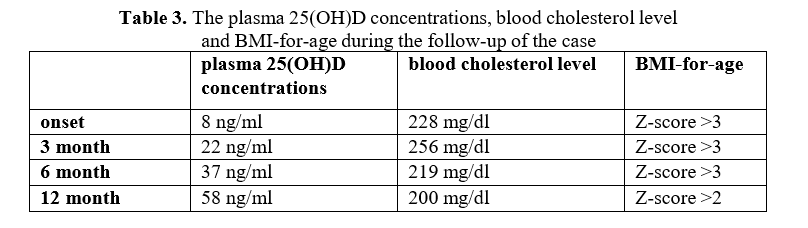
The biochemical assessment reveals low plasma 25-hydroxyvitamin D concentrations, high blood cholesterol level (in this situation familial hypercholesterolemia); the evaluation of respiratory function, by spirometry, shows a combined, restrictive and obstructive dysfunction.
After complete multidisciplinary assessment, the patient started a diet under nutritional counseling, in combination with kinetotherapy, psychological counseling and vitamin D-therapy; the basal treatment for asthma has been reassessed. clinical-biological surveillance was performed at 3 months, 6 months and 1 year after first presentation in our hospital (Table 3).
3. Results
Nutrient deficiencies are usually the result of dietary inadequacy, impaired absorption and use, increased requirement, or increased excretion. Vitamin D deficiency can occur when usual intake is lower than recommended levels over time, exposure to sunlight is limited, the kidneys cannot convert 25(OH)D to its active form, or absorption of vitamin D from the digestive tract is inadequate. Vitamin D-deficient diets are associated with milk allergy, lactose intolerance, ovo- vegetarianism, and veganism.
Milk is a major food for infant and young children and a lot of studies show us the impact of the type of milk consumed on nutrient intakes and nutritional status [2].
Serum concentration of 25(OH)D is the best indicator of vitamin D status. It reflects vitamin D produced cutaneously and that obtained from food and supplements [3].
Reference values for plasma 25-hydroxyvitamin D (25(OH)D) concentrations: Deficiency <10 ng/mL.
Insufficient level: 10-30 ng/mL Optimal level: 30-100 ng/mL Toxicity:> 100 ng/mL [4].
Because vitamin D is a fat-soluble vitamin, its absorption depends on the gut’s ability to absorb dietary fat. Individuals who have a reduced ability to absorb dietary fat might require vitamin D supplementation [5].
Food allergies are becoming increasingly prevalent, especially in young children. The risk factors in allergic disease are genetics, epigenetic dysregulation, microbial and dietary factors.
Cow’s milk allergy is commonly the first manifestation of food allergy and atopic march in an infant. Manifestations vary from mild to severe including anaphylaxis and can be IgE-mediated or non-IgE mediated.
Maternal and early-life vitamin D deficiency have notable influence on the susceptibility to food allergy, which may relate with the reduced population of Treg cell and the dysfunction of intestinal epithelial barrier [6]. In our case (case nr. 1), the mother did not receive vitamin D prophylaxis during pregnancy, but there is no biological assessment of vitamin D status for her. A new article reviews the current evidence for the experimental effects of vitamins A and D in vivo in animal models and on immune cells in vitro, and discusses their translational implication.
Vitamins A and D are able to modulate innate and adaptive immune responses and may therefore influence the development and the course of allergic diseases.
The authors concludes that animal studies predict that vitamin A and D may also be attractive players in the control of allergy in humans [7].
Several studies have observed an association between increasing latitude and food allergy prevalence, plausibly linked to lower ultraviolet radiation exposure and vitamin d synthesis in the skin [8]. More studies are needed to investigate the role of sunlight and vitamin d status in food allergy because of their potential for primary prevention and disease modification. [9], [10]
In the first case,vitamin D deficiency was due both to inappropriate nutrition in macronutrients and micronutrients, and to the associated pathology represented by cow’s milk allergy.
Normalization of the plasma 25-hydroxyvitamin D was achieved 3 months after the institution of vitamin D therapy, in combination with the diet corresponding to the underlying condition.
Calcium and vitamin D are important nutrients for child growth. Vitamin D is critical to phosphorus-calcium metabolism and to the growth and development of the skeleton. Optimizing vitamin D status is essential to optimize growth and achieving the maximum peak bone mass soon after the completion of adolescence [11].
Vitamin D deficiency has been widely reported in all age groups in recent years. Rickets has never been eradicated in developed countries [12]. The goal of treatment is to normalize vitamin D levels, to relieve symptoms and decrease the risk of fractures, falls, and other adverse health outcomes. To prevent vitamin D deficiency, the American Academy of Pediatrics recommends that infants and children receive at least 400 IU per day from diet and supplements [13].
For adolescents, the recommended dose is the same, in a vitamin complex or a unique vitamin D product, according to the American Academy of Pediatrics [14]. In addition to dietary sources, exposure to ultraviolet B sunlight provides children and adults with additional vitamin D. In the second case, substitution treatment with vitamin D in combination with a calcium-based preparation was initiated. The adolescent was clinically and biologically re-evaluated at 1 month and 3 months, when the symptomatology disappeared and the plasma concentrations of vitamin D and calcium return to normal.
Obesity is a significant health problem world-wide, particularly in developed nations. Accumulating evidence suggests vitamin D plays a role in the development of obesity and type 2 diabetes mellitus. Epidemiological studies have demonstrated that vitamin D deficiency is closely related to obesity and increased risk of type 2 diabetes mellitus, which are main chronic diseases harming human health [15]. Vitamin D deficiency is highly prevalent in overweight and obese children.
The particularly high prevalence in severely obese and minority children suggests that targeted screening and treatment guidance is needed [16]. A systematic review and meta- analysis published in 2015 concludes that the prevalence of vitamin D deficiency was more elevated in obese subjects.
The vitamin D deficiency was associated with obesity irrespective of age, latitude, cut-offs to define vitamin D deficiency and the human development index of the study location [17].
It is currently known that vitamin D has a number of biologic effects that are likely important in regulating key mechanisms in asthma. Vitamin D supplementation may lead to improved asthma control by inhibiting the influx of inflammatory cytokines in the lung and increasing the secretion of interleukin 10 by T-regulatory cells and dendritic cells [18].
Asthma exacerbations are favored by vitamin D deficiency and decrease after long-term vitamin D replacement [19]. Meta-analysis of a modest number of trials in people with predominantly mild to moderate asthma suggests that vitamin D is likely to reduce both the risk of severe asthma exacerbation and healthcare use [20].
In the third case, regarding plasma 25(OH)D concentrations, improvement was obtained after 3 months of treatment at therapeutic doses and complete correction at 6 months post-onset, level subsequently maintained within normal limits with prophylactic doses. The blood cholesterol level has remained above the normal age limits. Is known the importance of early cardiovascular risk assessment, and when the situation imposes it, and associating early drug therapy when necessary [21].
The multidisciplinary, planned approach has improved the BMI-for-age, the quality of life, pulmonary function and resistance to physical effort, which gives us hope for a significant improvement in the future, a chance for a healthy adult.
4. Conclusions
Knowing the implications of vitamin D in the body and the sensitive periods of growth and development, it is important to make biological determinations, in order to do proper prophylaxis and intervene promptly when changes occur. Prophylactic doses of vitamin D will be adjusted depending on the patient’s individual characteristics and on the risk factors for the occurrence of different pathologies.
It is important to periodically evaluate children and to administer the doses of prophylactic vitamin D correctly, because vitamin D deficiency are entirely preventable by routine supplementation. Always when hypocalcaemia is discovered, plasma levels of vitamin D should also be determined, especially when the patient associates other pathologies (respiratory, allergic, cardiac, bone).
Contributo selezionato da Filodiritto tra quelli pubblicati nei Proceedings “35th Balkan Medical Week - 2018”
Per acquistare i Proceedings clicca qui:
https://www.filodiritto.com/proceedings
Contribution selected by Filodiritto among those published in the Proceedings “35th Balkan Medical Week - 2018”
To buy the Proceedings click here:
