
Caesarean Section and Retinopathy of Prematurity


Abstract
Caesarean section (C-section) is a necessity, due to maternal and fetal pathology. In many developed countries, approximately one third of pregnant women give birth through caesarean section. The retinopathy of prematurity (ROP) is a multifactorial disease with invalidating potential. Multiple pregnancy, in vitro fertilisation, chorioamnionitis, low gestational age and birth weight, postnatal infections are risk factors that influence the development of the retinal vascularisation. The purpose of this study is to analyse whether the caesarean section may be considered a risk component for ROP. We analysed data from the charts of premature born in Polizu Maternity during 01.01.2016-31.12.2017 who underwent laser therapy for retinopathy of prematurity. All new-borns from the study had ROP stage 3+. About half of premature in the study were born through caesarean section. The maternal pathology is one of the most important factors which influence the type of birth.
Tablet of Contents:
1. Introduction
2. Methodology
3. Results
4. Conclusions
1. Introduction
Despite advances in perinatal and neonatal care, prematurity is still the major cause of mortality and long-term morbidity in infancy. Prematurity itself is the most important risk factor for retinopathy of prematurity (ROP), which is a vasoproliferative pathology occurring in premature with gestational age under 34 weeks. Retinal development is affected. Vascular growth at retinal level begins at 16 gestational weeks. Under the influence of risk factors that may lead to premature delivery (maternal age, in vitro fertilization, multiple pregnancy, preeclampsia, eclampsia, chorioamnionitis) and postnatal ones (low age and birth weight, supplemental administration of oxygen, sepsis, multiple transfusions for treating anemia, late onset of enteral nutrition etc.), the evolution of retinal vascularization is disturbed, leading to neovascularization. These new blood vessels can grow beyond normal levels, and without adequate ophthalmologic treatment, it can lead to retinal detachment and blindness. (1, 2, 3, 4, 5, 6, 7) ROP is classified by location (zone I, II and III) and severity (presence of plus factor) in 5 stages, from the mild form (stage 1) to the most severe one (stage 5) (1, 2, 3, 4, 5, 6, 7).
Screening of ROP must include premature under 34 gestational weeks and/or birth weight under 2000 grams, and those over 34 weeks with risk factors after birth (administration of oxygen with concentration over 40%, sepsis, necrotizing enterocolitis, anemia of prematurity, multiple transfusions, shock) (1, 2, 3, 4, 5, 6, 7, 21).
The indication of ophthalmologic treatment depends on the stage of ROP. The gold standard is laser intervention. (1, 2, 3, 4, 5, 6, 7)
Recently, studies have focused on identifying new antenatal risk factors for ROP, such as caesarean section delivery. This type of birth was meant to improve neonatal outcome especially for pregnancies in which maternal pathology has an impact on fetal viability. In cases of fetal damage, the caesarean section may reduce hypoxic stress, important risk factor for ROP. Studies aimed to determine whether caesarean section delivery has benefits for premature, but there were no statistically significant results. Despite having no evidence of advantages in neonatal outcomes and due to maternal and fetal pathology, cesarean section delivery is becoming more prevalent, particularly in early gestational ages. (8, 9, 10, 11, 12,15, 16, 17, 18, 20)
In the effort of reducing neonatal morbidity, maternal outcomes must be considered, when performing caesarean section. Studies found no benefit in very low birth weight infants but detected higher maternal morbidity. Controversies to establishing the ideal mode of delivery for preterm infants still exist, mainly because of population heterogenicity and clinical experience. (13, 14, 15, 16, 17, 18, 19, 20, 21).
2. Methodology
The study group includes 214 premature admitted in the Neonatology Clinic of N.I.M.C.H. Alessandrescu-Rusescu for laser therapy during 01.01.2016-31.12.2017. From this group, due to insufficient information, we chose to analyses only the premature born in Polizu Maternity.
In 2016 there were 12 interventions performed on premature delivered in our facility and in 2017-15. We analyzed gestational age, birth weight, sex, Apgar score, maternal pathology, mode of delivery, place of birth, resuscitation at birth, need of mechanical ventilation and existence of anemia of prematurity.
3. Results
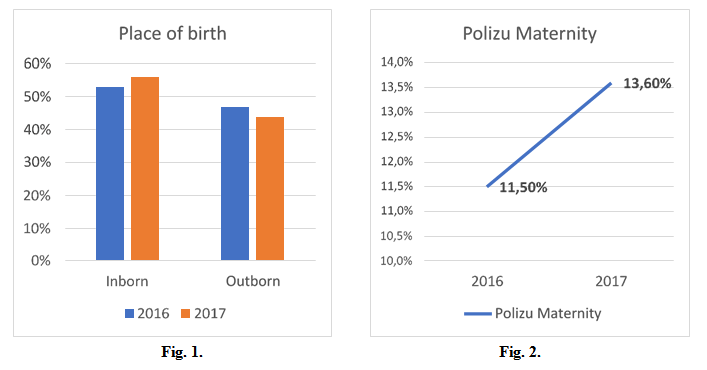
In the Neonatology Clinic of N.I.M.C.H. Alessandrescu-Rusescu, 53% of premature admitted for laser therapy ROP in 2016 came from level III maternities in Bucharest, in 2017, 56%. (Fig. 1)
In 2016, 11,5% of the premature with ROP who underwent laser therapy were born in Polizu maternity, in 2017, 13,6%. (Fig. 2)
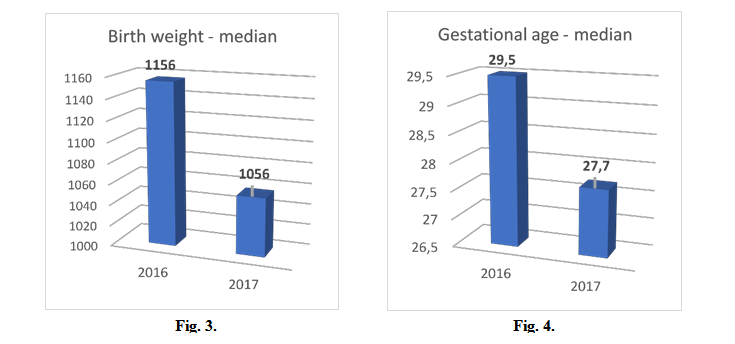
Median birth weight was 1156 grams in 2016, 1056 grams in 2017, with a minimum birth weight of 650 grams and maximum of 1350. (Fig. 3)
Median gestational age was 29,5 weeks in 2016, 27,7 weeks in 2017, with a minimum gestational age of 25 weeks and maximum of 31 weeks. (Fig. 4)
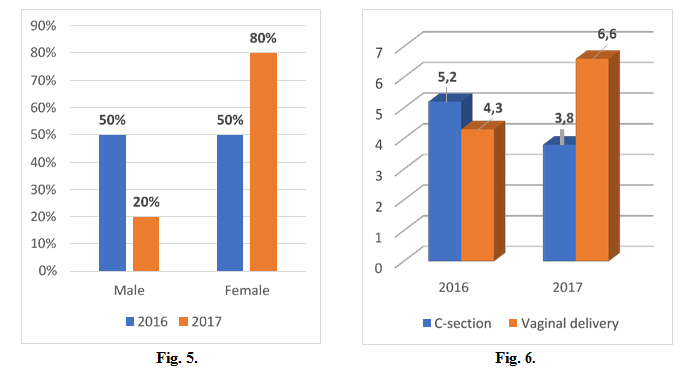
50% of the premature with ROP and laser therapy were males in 2016, 20% in 2017. (Fig. 5)
Median Apgar score was 5,2 (caesarean section) and 4,3 (vaginal delivery) in 2016, 3,8 (caesarean section) and 6,6 (vaginal delivery) in 2017, with a minimum of 1 and maximum of 7. (Fig. 6)
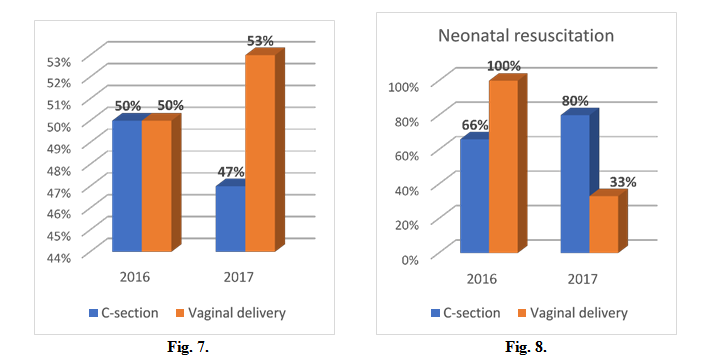
50% of premature in 2016 were delivered through caesarean section, 47% in 2017. (Fig. 7) Resuscitation at birth was performed in 66% of cases (caesarean section) and 100% (vaginal delivery) in 2016, 80% (caesarean section) and 33% (vaginal delivery) in 2017. (Fig. 8)
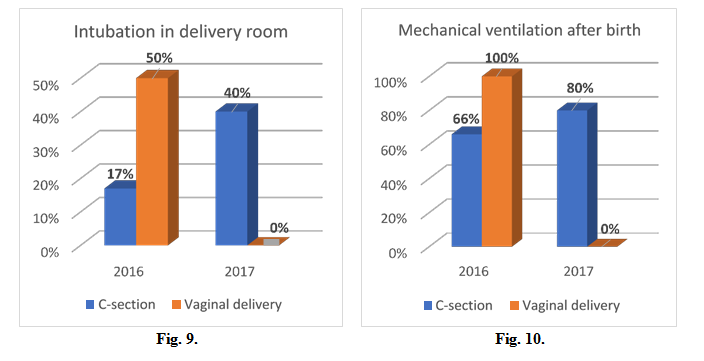
Intubation in delivery room was performed in 17% of cases (caesarean section) and 50% (vaginal delivery) in 2016, 40% (caesarean section) and 0% (vaginal delivery) in 2017. (Fig. 9)
Mechanical ventilation for respiratory distress syndrome was needed after birth in 66%% of cases (caesarean section) and 100% (vaginal delivery) in 2016, 80% (caesarean section) and 0% (vaginal delivery) in 2017. (Fig. 10)
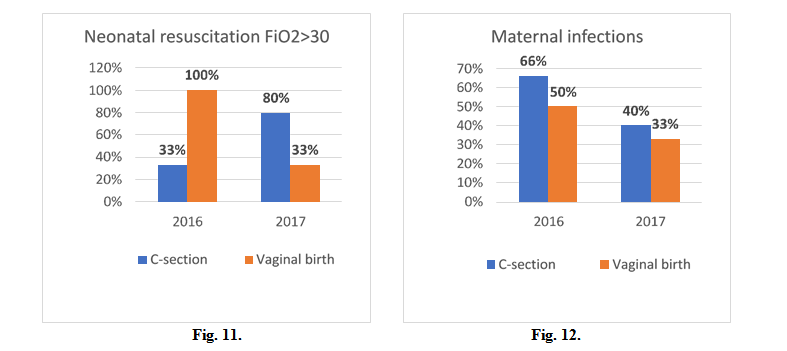
In 2016 a FiO2>30% was used in neonatal resuscitation in 100% of cases (vaginal birth) and 33% (caesarean section), in 2017 33% of cases (vaginal birth) and 80% (caesarean section). (Fig. 11)
In 2016 maternal infections were diagnosed in 50% of cases (vaginal birth) and 66% (caesarean section), in 2017 33% of cases (vaginal birth) and 40% (caesarean section). (Fig. 12)
Maternal and fetal pathology was heterogeneous (infections, vaginal bleeding, multiple pregnancies, in-vitro fertilisation, preeclampsia, eclampsia, placenta detachment, IUGR, umbilical cord prolapse, twin-to-twin transfusion syndrome), the most common being infections with different germs. The anaemia of prematurity was detected in all cases. All premature were diagnosed with retinopathy of prematurity stage 3+ before treatment (laser intervention).
4. Conclusions
Caesarean sections are usually performed for saving maternal and infant lives. This type of delivery should only be applied in precise medical circumstances. Up to this point, in literature, there is no evidence to support caesarean section as an optimal type of delivery in the case of premature.
The necessity of a caesarean section is established by maternal pathology, which has impact on fetal viability. Despite all this information, according to WHO, rates of cesarean section are rising. Although our studied group is not statistically significant, our data is similar to other studies that show caesarian section does not influence mortality in premature.
The Authors:
DATU Corina-Gabriela [1]
MOHORA Ramona [1] [3]
CRISTEA Octaviana [1] [3]
DATU Răzvan Constantin [2] [3]
[1] N.I.M.C.H. Alessandrescu-Rusescu-Polizu Maternity-Neonatology Clinic Bucharest (ROMANIA).
[2] E.C.H.C. Grigore Alexandrescu-Pediatric surgery Department Bucharest (ROMANIA).
[3] University of Medicine and Pharmacy “Carol Davila” Bucharest (ROMANIA).
Contributo selezionato da Filodiritto tra quelli pubblicati nei Proceedings “4th Congress of the Romanian Society for Minimal Invasive Surgery in Ginecology – Annual Days of the National Institute for Mother and Child Health Alessandrescu-Rusescu - 2018”
Per acquistare i Proceedings clicca qui.
Contribution selected by Filodiritto among those published in the Proceedings “4th Congress of the Romanian Society for Minimal Invasive Surgery in Ginecology – Annual Days of the National Institute for Mother and Child Health Alessandrescu-Rusescu - 2018”
To buy the Proceedings click here.
