
Pneumonia “Under Cover”

Abstract
Introduction
Pneumonia is a common infectious pathology which frequently has atypical clinical manifestations in elderly.
Case presentation
An 82-year-old man, known with chronic viral C hepatitis and hypertension, non-smoker, with no occupational exposure to noxes, presented for rest dyspnoea with orthopnoea, installed progressively over the last 2 weeks, bilateral leg edema and productive cough with ineffective expectoration. The patient was afebrile and denied fever, chills or chest pain. Relevant from the clinical examination: bilateral edema, perioral cyanosis, vocal vibrations diminished in the lower half of the left hemithorax, vesicular sounds present but diminished basal bilaterally with bilateral basal crackles. Para clinically the patient presented with a blood pressure of 160/90 mmHg, a heart rate of 85 bpm, mild leucocytosis with neutrophilia, respiratory alkalosis, hypocapnia and hypoxia.
The EKG showed synus rhythm, left ventricular hypertrophy and secondary terminal phase modifications. The abdominal ultrasound revealed only bilateral pleural effusion. Taking the clinical and paraclinical data into consideration, a clinical diagnosis of global heart failure syndrome was established, until the result of the thorax x-ray raised a high suspicion of a pulmonary tumour and a CT-scan was programmed. The CT examination infirmed the presence of a lung tumoral process and described an area of alveolar condensation with air bronchogram, the radiological aspect being highly suggestive of pneumonia. Under antihypertensive treatment, antibiotic and mucolytic treatment, the patient evolved favourably with symptom relief and radiological resolution.
Conclusions
It is a case of a community-acquired-pneumonia in a non-smoker, immunocompetent, elderly patient who had no fever, no chest pain and who presented with symptoms and clinical signs highly suggestive of cardiac failure, a case in which the radiological image played an important role for the final diagnosis.
Table of contents
1. Introduction
2. Case report
3. Discussions
4. Conclusions
1. Introduction
Pneumonia is a common lung infectious pathology that despite the continuous development of antimicrobial therapies remains a major cause of complications and death.
Community-acquired pneumonia develops in people without recent hospitalizations or regular exposure to the health- care system. The typical presentation of a community-acquired pneumonia consists in cough, dyspnoea, fever and pleuritic chest pain [1].
Advanced aged is associated with reduced symptoms, the absence of fever being frequently reported, especially in patients over 80 years [2].
2. Case report
We present a case of an 82-year-old man, known with chronic viral C hepatitis and untreated hypertension, non-smoker, with no occupational exposure to noxes, who presented at the emergency room for rest dyspnoea with orthopnoea, installed progressively over the last 2 weeks, bilateral leg edema and productive cough with ineffective expectoration. The patient was afebrile and denied ever having fever, chills or chest pain.
Relevant from the clinical examination: bilateral leg edema, perioral cyanosis, vocal vibrations diminished in the lower half of the left hemithorax, vesicular sounds present but diminished basal bilaterally with bilateral basal crackles, blood pressure of 160/90 mmHg, a heart rate of 85 bpm. Para clinically, the patient presented with mild leucocytosis with neutrophilia, respiratory alkalosis, hypocapnia and hypoxia.
The ECG showed synus rhythm, left ventricular hypertrophy and secondary terminal phase modifications. The abdominal ultrasound revealed only bilateral pleural effusion. Taking the clinical and paraclinical data into consideration, a clinical diagnosis of global heart failure syndrome was established and the patient received antihypertensive and diuretic medical therapy.
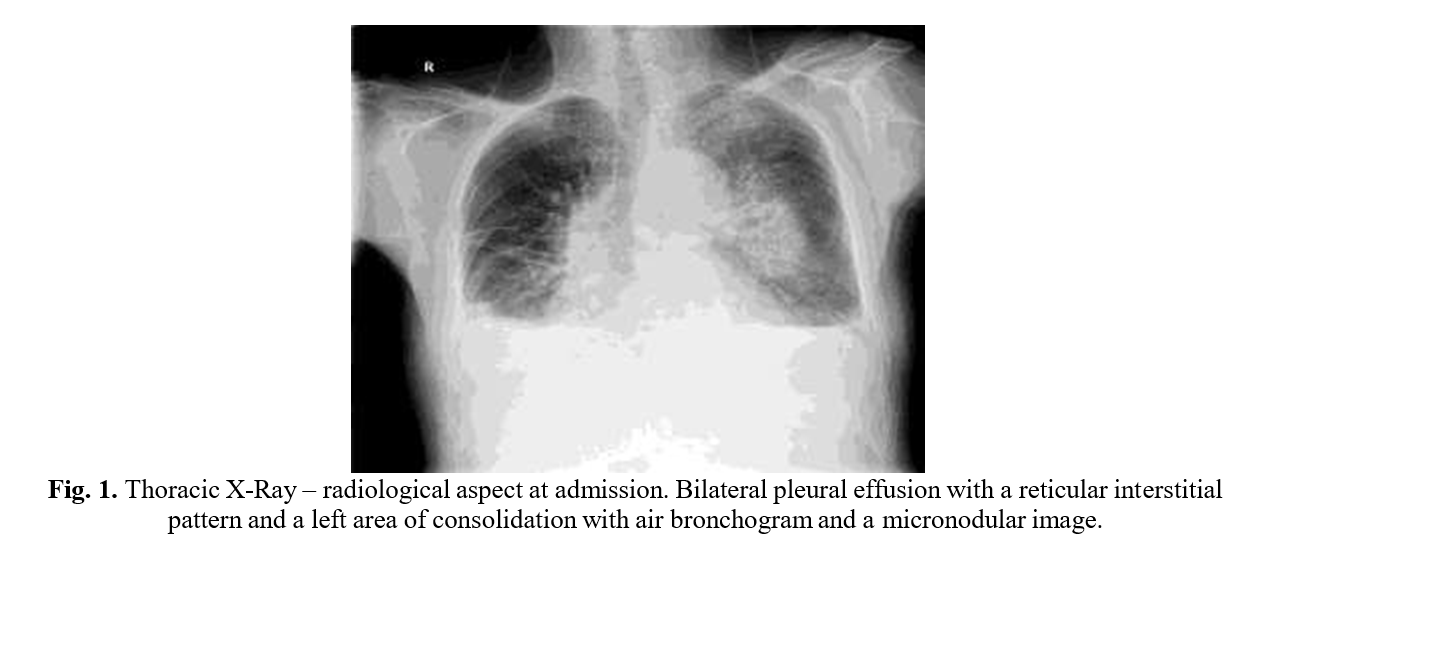
The result of the thorax X-ray (Fig. 1) changed the medical approach for this patient, raising a high suspicion of a pulmonary tumour. The patient was admitted to the hospital and a CT-scan was programmed.
With antihypertensive and diuretic drugs, the leg edema reabsorbed, but the productive cough and dyspnoea persisted. The patient had his body temperature, blood pressure and heart rate followed until the CT-scan.
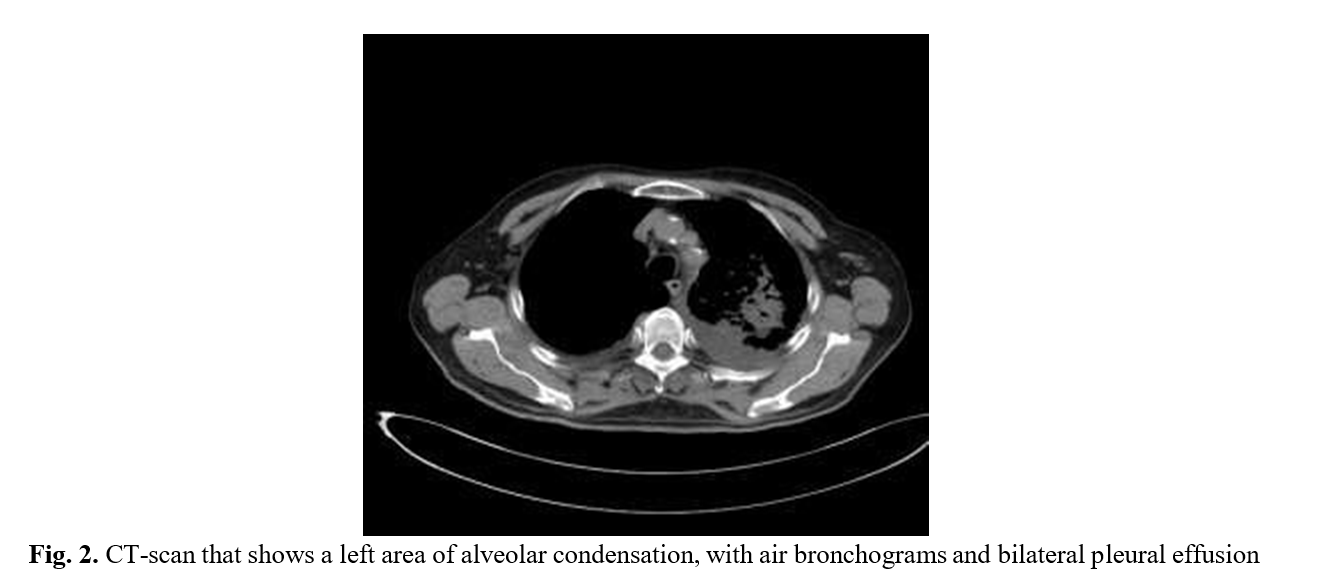
The CT examination (Fig. 2) infirmed the presence of a lung tumoral process and described an area of alveolar condensation with air bronchogram, the aspect being highly suggestive of pneumonia.
After the result of the CT-scan, the patient has also been given antibiotics and mucolytics, having a favourable clinical and paraclinical evolution, with the reduction of cough and dyspnoea.
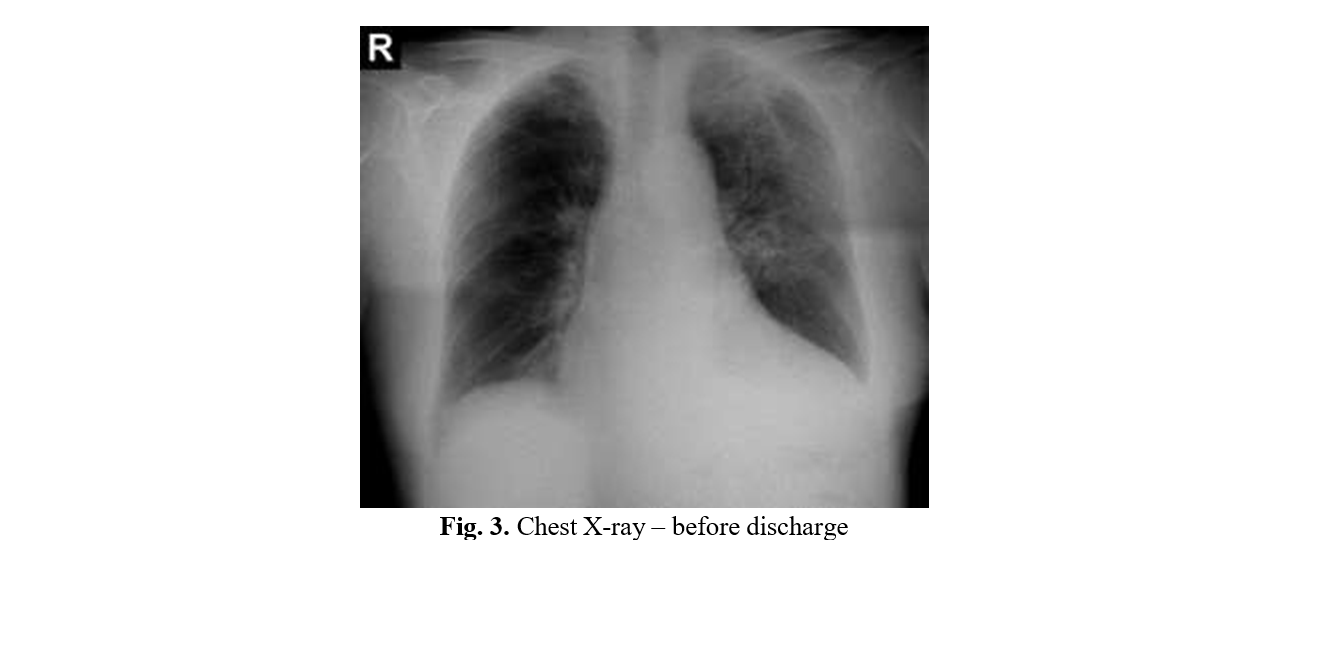
Before the discharge, a control X-ray was performed that showed radiological resolution (Fig. 3).
3. Discussions
Pneumonia, even if a frequent infectious pathology, is sometimes difficult to diagnose, especially in the elderly patients, because of the atypical clinical presentation in this subgroup of patients. Sometimes, pneumonia can be encountered as a paraneoplastic syndrome [3-7] or it can appear like a complication of a minor surgery [8-12].
This particular patient presented with signs and symptoms highly suggestive of heart failure.
He had a medical history of therapeutically neglected hypertension and presented with bilateral leg edema, cough associated with exertional dyspnoea and high values of the blood pressure.
The ECG findings supported this diagnosis, showing left ventricular hypertrophy, a common finding among the patients known with hypertension [13].
High grade fever associated with chills is a frequent symptom in patients with typical pneumonia [14, 15], but may be absent in cases of atypical pneumonia [16], in immunocompromised patients [17] or in elderly [18, 19]. This patient was afebrile and denied ever having fever or chills.
4. Conclusions
The only aspect of the clinical examination of this patient that suggested a pneumonia was the productive cough. In an elderly patient, the diagnosis of pneumonia has to be taken into consideration, despite the absence of fever or pleuritic chest pain.
Contributo selezionato da Filodiritto tra quelli pubblicati nei Proceedings “35th Balkan Medical Week - 2018”
Per acquistare i Proceedings clicca qui:
https://www.filodiritto.com/proceedings
Contribution selected by Filodiritto among those published in the Proceedings “35th Balkan Medical Week - 2018”
To buy the Proceedings click here:
